Further reducing child mortality requires improving primary care infrastructure across a continuum for women, newborns, and children, allowing for the successful dissemination of interventions known to be effective for the major causes of maternal, newborn, and child mortality. The following recurrent themes emerge in the description of progress addressing the major causes of child mortality:
- A need to strengthen and improve community-based services for a greater effect on diseases (ie, pneumonia, diarrhea, malaria)
- A need to address the inequities of how effective interventions are being disseminated among people of different socioeconomic statuses and urban versus rural
Pneumonia
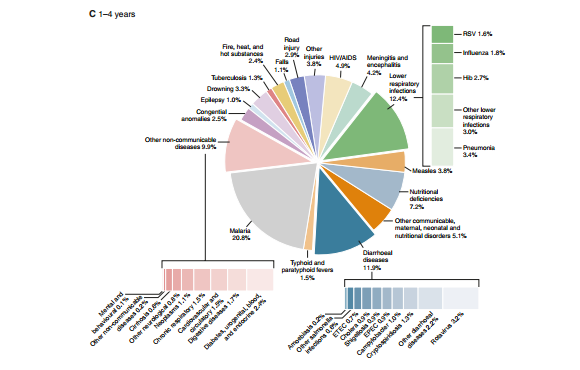
Pneumonia is associated with 18% or 1.2 million childhood deaths every year, a number greater than deaths from malaria and diarrhea combined and the number one cause of death in children younger than 5 years globally. Morbidity from pneumonia is estimated at 156 million cases annually. Ninety percent of pneumonia deaths occur in South Asia and sub-Saharan Africa.The pathogens S pneumoniae, Hib, respiratory syncytial virus, and influenza cause the majority (estimated at 55%) of pneumonia deaths, while household air pollution and overcrowding are environmental contributors.It is estimated that 3 billion people use solid fuel for cooking (wood, crop waste, coal), contributing to indoor pollution .
Together, pneumonia and diarrhea account for almost 30% of deaths in children younger than 5 years; several of the most effective interventions to combat these diseases overlap, including improved nutrition, breastfeeding, and zinc therapy. In April 2013, the World Health Organization (WHO), UNICEF, and Joint United Nations Programme on HIV/AIDS (UNAIDS) launched the Global Action Plan for Pneumonia and Diarrhoea (GAPPD). It is a framework for governments to plan and implement effective interventions for prevention and control of both diseases; this is one of the biggest opportunities in global health. Scaling up these activities could prevent 95% of diarrhea deaths and 67% of pneumonia deaths by 2025.The current global health approach to decreasing deaths from pneumonia involves prevention and early detection with prompt treatment.
 |
Indoor Air Pollution (picture of child exposed to indoor smoke)
A young child sits over a cooking fre inside his family’s hut in the Awer IDP camp in northern Uganda’s conflict-affected district of Gulu.
|
Early Detection and Treatment
It is essential to educate and encourage families to seek care early in the course of respiratory illness; the IMCI program is an ideal conduit for education and treatment. First, families can be taught to observe respiratory rates and chest wall appearance (eg, in-drawing). The IMCI program workers can also look at these physical signs, refer severe cases, and treat non-severe cases with selective antibiotics.Statistics show that worldwide, too few people know to access care when their child is ill with respiratory symptoms. Only 60% of caregivers worldwide seek care, with little progress over the last decade (54% sought care in 2000).This number is even lower in sub-Saharan Africa (49%).Only one-third of those needing antibiotics are getting them. The case management approach also suffers due to a lack of caregivers, inadequate training and program coordination, and trouble with the supply chain for items such as antibiotics. While most countries agree that case management is important, the number of countries who implemented the policy to scale, reaching all children, is few ; thus, more work must be done to expand the reaches of the IMCI program.
 |
| Community Case Management Policy |
Prevention
Not only can IMCI workers instigate prompt treatment, they can also encourage breastfeeding, improved nutrition (including increased zinc intake), and hand washing. Human milk can provide antibodies as well as have a positive economic and social effect on families. All-cause mortality increased 566% in infants 6 to 11 months and 223% in children 12 to 23 months who were not breastfed.
Expanded use of Hib, pneumococcal, pertussis, measles, and influenza vaccines is also an important approach to decreasing childhood pneumonia.H influenzae type b vaccination is very effective in Kenya, where the incidence of the disease decreased to 12% of its baseline level in children younger than 5 years over the frst 3 years it was distributed.For years, access to Hib vaccine demonstrated a rich/poor gap between countries. Thankfully, that gap is closing, owing to an increase in funding as well as global and national leadership. In 2000, Gavi, the Vaccine Alliance, began fnancially supporting Hib vaccination in 72 of the poorest countries. Countries apply for Gavi funding based on a fnancial plan, vaccine introduction plan, and 5-year national vaccine strategy. Initially, uptake of Hib vaccine was very slow. When the Hib Initiative was launched in 2005 to accelerate introduction of the Hib vaccine, there was a sharp increase in the number of eligible countries using the vaccine . Eighty-fve percent to 90% of all-income countries introduced the Hib vaccine by the end of 2011. Since 2007, WHO has recommended global use of pneumococcal vaccine, especially because pneumococcus is the leading cause of pneumonia globally. It is estimated that 500,000 child deaths could be averted annually with the use of pneumococcal vaccine.While the uptake
 |
| Closing the Rich/Poor Gap in the Introduction of Haemophilus influenzae Type b Vaccine in Recent Years |
of pneumococcal vaccine globally is slowly rising, there are signifcant numbers of unimmunized children and a large gap in access between the rich and the poor.Hopefully, with initiatives (ie, advance market commitment) intended to lower vaccine prices and increase distribution, the fnancing and organizational mechanisms that improved Hib vaccine uptake will also lead to expanded coverage of pneumococcal vaccine.
Diarrhea
Diarrhea is responsible for 11% (750,000) of child deaths annually worldwide.Fortunately, signifcant strides have been made in diarrhea control over the last 15 years. Rotavirus, enteropathogenic Escherichia coli, calicivirus, and enterotoxigenic E coli cause more than 50% of severe diarrhea episodes (ie, those most likely to result in death). It is estimated that rotavirus causes 38% of diarrheal deaths.Diarrheal control and decreases in mortality are achieved through prevention and also adequate treatment during the illness. One of the leading success stories in public health is the use of oral rehydration therapy (ORT) as a key element in fghting diarrhea. Oral rehydration therapy is associated with a 69% decrease in mortality. Deaths caused by diarrhea decreased by more than two-thirds since 1980; diarrhea is no longer the number one cause of death.
The GAPPD goal is to decrease mortality from diarrhea to fewer than 1 per 1,000 live births and have 90% case management coverage by 2025. Treatment includes ORT, continued feeding (especially human milk for young children), and zinc.Prevention includes safe water supply, feces disposal (MDG 7), hand washing, immunization (for rotavirus and measles, specifcally), and improved nutrition (including adequate vitamin A). Stunting, a chronic marker of malnutrition, occurs when there are repeated diarrhea episodes, setting up a vicious cycle of undernutrition and infection that needs to be broken.
Oral rehydration solution (ORS) is the mainstay of ORT. Oral rehydration solutions evolved over time and now are composed of a lower salt concentration than previously recommended in the 1980s and 1990s. Homemade rehydration solutions are loosely encouraged in regions where ORS is not available. Zinc has become an important adjunct to diarrhea control. It is estimated that 17% of the world’s population is zinc defcient.While ORS acts to rehydrate, zinc decreases the amount of diarrhea and length of illness.In addition to ORS and zinc, families are encouraged to continue feeding and increase fluids in general. Unfortunately, treatment use slowed after an initial dramatic rise in the uptake of rehydration recommendations in the early 1990s.24 Overall, only about 34% of children with diarrhea receive low-osmolar ORS and only 5% get zinc; however, there are regional variations.24 Treatment inequities occur depending on socioeconomic status: children are 1.5 times as likely to receive treatment in households with higher income levels. There are also urban/rural inequities: those in urban settings are more likely to receive treatment than those in rural areas (43% versus 34%).
Prevention
Integrated Management of Childhood Illness workers promote hand washing, which is estimated to decrease the rate of diarrheal morbidity by 42%.However, the poorest households do not have access to necessary soap and water.Globally, the MDG to achieve safe drinking water was met (a huge success), but access in rural areas is often still poor. Sanitation has also been improved but, again, less so in rural areas. Improved nutrition also helps decrease severity of diarrhea illness; exclusive breastfeeding for the frst 6 months of life is encouraged and then continued breastfeeding until 2 years of age along with other solid food.
Because rotavirus infection is the leading cause of severe-acute diarrhea worldwide, an important consideration is an effective rotavirus vaccine. The WHO now recommends rotavirus vaccine worldwide, especially in South Asia and sub-Saharan Africa, where the burden of disease is the greatest. The goal for 2015 is that Gavi can provide monetary assistance to 40 of the world’s poorest countries to introduce the rotavirus vaccine.As of 2011, rotavirus vaccine was basically unavailable in low-income countries.
To make headway with diarrhea, there must be an increase in funding, policy changes, collaboration between public and private organizations, government support, and adequate supply and uniform distribution of ORS and zinc.Bangladesh is a model country for what can be done; mortality from diarrhea is at 2% (down from 20% in 1993) and almost 80% of people are receiving ORS and 33% are receiving zinc.
Injury
Injury and violence are major killers of children throughout the world, responsible for approximately 950,000 deaths each year in children and adolescents younger than 18 years.25 Unintentional injuries account for almost 90% of these cases and are the leading cause of death for children aged 10 to 19 years. demonstrates that as children age, the proportion of deaths attributable to injury, compared with communicable and noncommunicable disease, increases. The majority of these injuries are the result of road traffc collisions, drowning, burns (fre or scalds), falls, or poisoning. These 5 categories of unintentional injuries
 |
Proportion of Deaths From Injuries, Noncommunicable Diseases,
and Communicable Diseases, by Age, Among Children in the World, 2004 |
make up 60% of all child injury deaths. Road traffc injuries alone are the leading cause of death among 15- to 19-year-olds and the second leading cause among 10- to 14-year-olds.
Other unintentional injuries include suffocation, asphyxiation, choking, animal bites or snakebites, hypothermia, and hyperthermia. This group accounts for 23% of childhood deaths, which is a signifcant proportion. The rate of child injury death is 3.4 times higher in lowand middle-income countries than in high-income countries, but there are large variations in the injury-related death category. For fre-related deaths, the rate in low-income countries is close to 11 times higher than in high-income countries, drowning is 6 times higher, poison is 4 times higher, and falls are around 6 times higher.
Burden of injury is heaviest among the poor in countries with lower incomes. Overall, more than 95% of all injury-related deaths in children occur in low- and middle-income countries. Although the child injury death rate is much lower among children from developed countries, injuries are still a major cause of death, accounting for approximately 40% of all child deaths.
Many children who survive death are disabled from nonfatal injuries, often with lifelong consequences. Road traffc injuries and falls rank in the top 15 causes of disability-adjusted life years lost for children 0 to 14 years of age.
Survey data from Bangladesh, China, the Philippines, Thailand, and Vietnam show that suffocation is the main cause of injury-related death in children younger than 1 year; drowning is the main cause of injuryrelated death in children younger than 5 years; drowning, road traffc injuries, and animal bites are the main cause of injury-related death for children between 5 and 9 years; and road traffc deaths are the most signifcant unintentional injury among children 10 to 17 years of age. However, there are large differences between rich and poor countries. While drowning is the leading cause of injury death among children younger than 5 years in the United States and Asia, the rate of death per 100,000 children is 30 times higher in Asia.
In an analysis of child death rates by gender, male deaths exceed female deaths in nearly all mechanisms of injury, with the exception of fre-related burns. Excess deaths from fre-related burns among females is particularly noticeable in the Southeast Asia region and low- and middleincome countries of the Eastern Mediterranean region, where female adolescent deaths can exceed adolescent male death by up to 50%.7 Male death rates are one-third higher than female death rates in children 5 to 9 years of age, a discrepancy that increases to 60% among children 10 to 14 years of age. Adolescents 15 to 17 years of age show an adult profle; males in this age group account for more than 86% of all injury-related deaths, particularly in high-income countries.
Prevention
Injuries are not accidents—they are not inevitable. The global community now recognizes that most child injuries are predictable and preventable. In Organisation for Economic Co-operation and Development countries, for example, the number of injury deaths among children younger than 15 years fell by half between 1970 and 1995. Preventing child injury is closely connected to other issues related to children’s health, including poverty, inequality, the built environment (eg, housing stock, water access, cultural practices, quality of roads and vehicles), and personal protective behaviors (eg, seat belts, motorcycle helmets, child supervision).
Child injury prevention can be a central part of all initiatives to improve child mortality. Every child death is a loss to the country’s future economy. Injury prevention will reduce costs in the health care system, improve country capacity to meet its development goals, and, most importantly, improve the chances of children living a long, productive, and healthy life. Unless injury prevention is included in child survival programs, children will grow up subjected to injuries, and the effect of large investments in immunization, nutrition, and maternal and child health care may be lost.
Malari
More than 600,000 annual deaths are ascribed to malaria, of which the majority are in sub-Saharan Africa. Forty percent of all deaths occur in just 2 countries: the Democratic Republic of Congo and Nigeria. Children younger than 5 years comprise 91% of the malaria victims; this essentially equates to one child dying every minute from the disease.Malaria is the number one killer of children in the sub-Saharan region, exceeding the number of children who die from pneumonia . Malaria also causes signifcant morbidity; recurring infections can lead to chronic anemia and impaired growth and development. Perinatal infection causes low birth weight.
From 2000, when 44 African leaders signed the Abuja Declaration to cut malaria deaths in half, to 2010, 1.1 million lives were saved and mortality rates declined by 33%. Fifty countries are on track to decrease malaria incidence by 75% by 2015. Increasing attention to the fght against malaria is also reflected in increased funding, from $100 million annually in 2000 to $1.7 billion in 2010, which is attributable to such groups as the Global Fund to Fight AIDS, Tuberculosis and Malaria; World Bank Booster Program for Malaria Control in Africa; and US President’s Malaria Initiative.
Malaria control has centered on prevention (vector control), early detection, and prompt treatment.Prevention includes long-lasting insecticide-treated nets (LLINs) (formerly called insecticide-treated bed nets). If used regularly, LLINs decrease mortality in children by 20%. Bed nets not only protect the individual using it but also those individuals in close proximity because of their insecticidal or repellent effects. An innovative and highly effective approach is to combine LLIN distribution programs with other interventions such as immunization.In 2005, LLINs were distributed as an adjunct to a polio campaign in Niger, which resulted in disseminating 2 million LLINs and increasing ownership from 6% to 70%.32 Bed net ownership in Africa varies from 30% to 80% of households, depending on the country. Bed net ownership for children increased from less than 5% in 2000 to more than one-third in 2012.28 It is also a goal to reach pregnant women with this preventive measure, for which success varies from less than 40% coverage to as high as 70%. Protection is even greater when LLINs are combined with indoor residual spraying; their combined use is promoted where funding allows.
Families are encouraged to seek early care for their febrile ill-appearing child by medical workers or IMCI staff who are able to provide prompt and early treatment. A recent Nigerian study shows some of the barriers to care seeking. Mothers frequently wait to see if the disease truly is malaria and will then use home remedies from a dealer rather than a clinic. Many also must wait for their husband’s decision to seek care. Families are encouraged to seek early care for their febrile ill appearing child by medical workers or IMCI staff who are able to provide prompt and early treatment. A recent Nigerian study shows some of the barriers to care seeking. Mothers frequently wait to see if the disease truly is malaria and will then use home remedies from a dealer rather than a clinic. Many also must wait for their husband’s decision to seek care.
The 2010 WHO recommendation calls for universal diagnostic testing when available and discontinuing empiric treatment. Malaria is now treated with artemisinin combination therapies, which are the only effective treatments due to increasing parasite resistance. These medications are expensive and quantity is limited; thus, the recommendation is to use them only if the illness is documented. Rural areas currently lag behind in access to diagnostic testing.
Preventive intermittent treatment during pregnancy in endemic areas (2 doses of an antimalarial drug in the second and third trimester) is another element in the fght against malaria. This treatment considerably reduced the number of women with anemia as well as the incidence of placental malarial infection and low birth weight.35 The number of women receiving preventive intermittent treatment during pregnancy increased in the last 10 years but still ranges from 5% to 70%, depending on the country.
HIV
The HIV/AIDS epidemic directly and indirectly affects children. Children not only contract HIV, but they are adversely affected when they live with family members, especially parents or other caregivers, who are infected. These children may be left responsible for heading households and earning wages to support their family. Children lose access to education, health care, and adequate food supplies in the many communities where teachers, health care workers, and farmers are infected with HIV. It is estimated that more than 17.8 million children worldwide have lost at least one parent to HIV. The HIV epidemic dealt a severe blow to child mortality progress, not only directly because of child deaths but also because of the necessity of redirecting resources to deal with HIV and its fallout. The resulting economic disruption of countries further contributed to malnutrition and poor health among the children in affected communities.
While the total number of people living with HIV increased over the last decade, the increase reflects longer life expectancy because more people are accessing treatment. The number of new cases actually
 |
Malaria Deaths Among Children Younger Than 5 Years in Africa (as percent
of younger-than-5 deaths) |
declined (incidence decreased by 33% since 2001; 2.3 million new cases in 2012), as has the number of deaths (down by 30%).
Sub-Saharan Africa is still the most severely HIV-affected region. Of the 35.3 million people infected with HIV, 70% live in sub-Saharan Africa (25 million), including the majority (88%) of the 3.4 million children who are infected with HIV.
The majority of children infected with HIV (90%) acquire the infection perinatally or through breastfeeding. Without perinatal medicines, risk of HIV transmission from mother to child is 15% to 30%; with prolonged breastfeeding, the transmission rate can be as high as 45%.
However, UNAIDS reports signifcant progress. In 2012, 62% of pregnant women received antiretroviral treatment, compared with only 9% in 2004. As a result, new pediatric HIV infections declined by 35% between 2009 and 2012.Four of the priority countries already achieved the goal of 90% coverage by 2015: Botswana, Ghana, Namibia, and Zambia. Botswana is an example of how political will has the power to produce change. This country put a high priority on screening programs—the president of Botswana declared that all women in antenatal clinics would be screened unless they refused; subsequently, the screening rate of women jumped to 90%.











{kind=link}