“We have an opportunity to focus global attention on what should be obvious: every mother, and every child, counts. They count because we value every human life. The evidence is clear that healthy mothers and children are the bedrock of healthy and prosperous communities and nations.”— Dr LEE Jong-wook, former World Health Organization Director-General
CURRENT STATUS OF CHILD MORTALITY
Global child mortality has signifcantly decreased in the last 20 years from 12.6 million deaths per year in children younger than 5 years in 1990 to 6.6 million deaths per year in 2012. The younger than-5 mortality rate has decreased by 47% since 1990 from 90 deaths per 1,000 live births to 48, and the decline rate is accelerating.1 Of the 61 countries with the highest mortality, 25 decreased their child mortality rate by more than two-thirds, including successes in Bangladesh (72%), Malawi (71%), and Nepal (71%). Despite these great strides, 18,000 children die every day—the majority from preventable causes.1 Deaths are increasingly concentrated in neonates (now 40% of all child deaths), as global public health efforts have resulted in declines in the mortality rate among older infants and children. Figure 1-1 shows the primary causes of global child mortality, including neonatal causes, pneumonia,
 |
| Global Distribution of Deaths Among Children Younger Than 5 Years, by Cause, 2012 |
However, global statistics fail to describe the great inequality of childhood mortality rates from country to country. While child mortality has declined in all regions of the world, the rate of decline is much slower in sub-Saharan Africa and South Asia, and it is in these regions that the greatest burden of child mortality is increasingly concentrated. Sub-Saharan Africa continues to have the highest mortality rate (98 per 1,000 live births), which is double that of other developing regions and 16 times more than developed countries.1 Child death is also disproportionately seen in rural areas among children whose mothers are not educated and those living in poverty and war-torn regions.1 There is also regional variation in childhood death patterns. Malaria is the primary killer of children younger than 5 years in Sub-Saharan Africa; while infectious diseases account for 64% of deaths globally, they are responsible for 81% of the deaths in Africa. More than half of deaths caused by infections can be ascribed to 5 pathogens: Plasmodium falciparum, Streptococcus pneumoniae, rotavirus, measles, and Haemophilus influenzae type b (Hib).2
'
 |
| Children in Sub-Saharan Africa and Southern Asia Face a Higher Risk of Dying Before Their Fifth Birthday |
GLOBAL BURDEN OF DISEASE 2010
Statistics of global health for people of all ages have been examined independently by the Global Burden of Disease Study 2010, funded by the Bill & Melinda Gates Foundation. This comprehensive data summary includes 235 causes of morbidity and mortality for people of all ages and looks at causes of death and trends in morbidity and mortality from 1990 to 2010.5 The overall global trend across all ages is a movement away from maternal, neonatal, nutritional, and communicable causes of death to noncommunicable causes, such as ischemic heart disease, stroke, lung cancer, and injury. This trend is driven by population growth and aging. Deaths related to diabetes doubled, and the number of deaths from road traffc crashes rose by 46%. Yet the picture can look quite different regionally. Specifcally, communicable diseases and maternal, neonatal, and nutritional causes of mortality account for 76% of deaths in sub-Saharan Africa. Figures 1-3a,b,c show the primary
{kind=link}
 |
| Global Burden of Disease Study—Neonates (0–27 Days) |
 |
| Global Burden of Disease Study—Infants (<1 Year) |
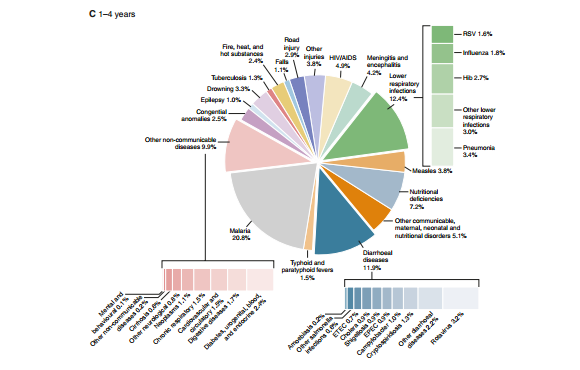 |
| Global Burden of Disease Study—Children (1–4 Years) |
causes of death (both sexes combined) for neonates, infants younger than 1 year, and children 1 to 4 years of age.
MILLENNIUM DEVELOPMENT GOALS FOR 2015
In 2000, 189 governments and at least 23 international organizations convened at the UN Millennium Summit to adopt a uniform worldwide set of 8 goals—Millennium Development Goals (MDGs)—to promote continued progress toward improving global public health. Several of these goals pertain to child health. Millennium Development Goal 4 sets the goal to decrease the mortality of children younger than 5 years to 5 million per year by 2015. Essentially, successful implementation of MDG 4 will decrease deaths by two-thirds of the levels seen in 1990 (13 million).
Other MDGs will indirectly improve child mortality rates. For example, MDG 5 is aimed at reducing maternal mortality by three fourths (which will affect neonatal mortality), and MDG 6 strives to reverse the spread of HIV/AIDS and malaria.6 While injury prevention was not part of the original MDG, Anupama Rao Singh, regional director of United Nations Children’s Fund (UNICEF) East Asia and Pacifc, points out, “If we are ultimately going to meet the Millennium Development Goal to reduce child mortality, it is imperative that we take action to address the causes of childhood injury.”
The MDGs are a valuable benchmark intended to move the world forward. Despite the overall decline in child mortality, only 23 of the 75 Countdown countries are on track to achieve MDG 4. These 75 Countdown countries carry 95% of the burden of maternal, newborn, and child death. Their progress is monitored as the world “counts down” to 2015. The current rate of decline needs to accelerate if we are to achieve the 2015 goal .
 |
| Younger-Than-5-Years Mortality Rate, 1990–2012, and Projected Rate, 2013–2028 (rate of decline and required rate of decline for Millennium Development Goal 4) |
I'm here to give my testimony how I was cured from HIV, I contacted my HIV via blade. A friend of my use blade to peel of her finger nails and drop it where she use it, so after she has left i did know what came unto me i looked at my nails, my nails were very long and I took the blade which she just used on her own nails to cut of my finger nails, as i was maintaining my names, i mistakenly injured myself. I did even bother about it, so when I got to the hospital the next week when i was ill the doctor told me that I am HIV positive, i wondered where did i got it from so i remembered how I use my friend blade to cut off my hand so i feel so sad in my heart to the extent that i don’t even know what to do, so one day i was passing through the internet i met a testimony of a lady that all talk about how she was cured by a doctor called DR Imoloa so i quickly emailed the doctor and he also replied to me and told me the requirements which i will provide and I do according to his command, he prepare a herbal medicine for me which I took. He message me the following week that i should go for a test which i did to my own surprise i found that i was HIV negative. He also have cured for all kinds of incurable diseases like: Huntington's disease, back acne, chronic kidney failure, Addison's disease, Chronic Disease, Crohn's Disease, Cystic Fibrosis, Fibromyalgia, Inflammatory Bowel Disease, Fungal Nail Disease, Paralysis, Celia Disease , Lymphoma, Major Depression, Malignant Melanoma, Mania, Melorheostosis, Meniere's Disease, Mucopolysaccharidosis, Multiple Sclerosis, Muscle Dystrophy, Rheumatoid Arthritis, Alzheimer Disease and so many. Thanks to him once more the great doctor that cured me dr. Imoloa so you can also email him via drimolaherbalmademedicine@gmail.com or what'sapp him on +2347081986098.. God Bless you Sir.
ReplyDelete